
Process – The Neglected Continuum in Healthcare
Category : Healthcare
OVERVIEW | METHODOLOGY | RESULTS | CONCLUSIONS | COMMENTARY
OVERVIEW
Electronic Health Records (EHR) solutions have been much maligned. They havedoc8c been credited for everything that is right and blamed for everything that is wrong about healthcare. CEOs and CIOs have lost their jobs over failed implementations. Recently an EHR was partially blamed for allowing a patient to leave a Texas hospital with the Ebola virus. People would be better served looking at the total roadmap for any technology transformation which includes 3 interrelated continuums – technology, people and process and recognize the EHR is actually just part of the solution.
Organizations have put a lot of money and effort behind the technology and the training of the people, but sometimes the process design, redesign or workflow is slighted. An ethnographic research study found that inefficient or poorly designed processes can be a contributing factor in many implementation failures; in this case, physician engagement. Our goal was initially to observe how physicians interacted with the solution; we learned a lot more than was planned.
Ethnography is a qualitative research method that tells a story from the perspective of those being researched. It is always conducted in the field and typically involves some sort of participant observation in which the researcher actually gets involved with the activities being studied by watching how people use products in their own environments, talking to them, and asking them questions. In this case, the researchers were trained and embedded in the various hospital units as physician support personnel to help them learn how to enter computerized patient orders.
METHODOLOGY
The study took place at a multi-hospital system in suburban Chicago. The system has about 1,000 physicians on staff and with privileges. The goal was to understand the challenges to physician engagements during implementation of a computerized physician order entry system. The EHR system was one of the top solutions but not the leading solution. This minimized any ‘halo effect’ from physicians’ acceptance just because it was the leading solution.
The study observed over 600 of the 1,000 physicians as they entered orders in almost all hospital units including: intensive care, transitional care, telemetry, cardiac care, catheter lab, day surgery and labor and delivery. Physicians observed were from a variety of specialties, including: internal medicine, cardiology, oncology, hematology, neurology and cardiovascular surgery. The study produced 125 representative comments and behaviors. The same or similar comment or behavior may have been observed by multiple physicians.
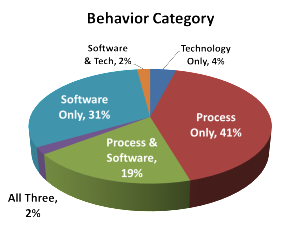
Observations were classified into three categories: process (how something is done), system (the EHR solution) or technology (the physical hardware or solution access). Some observations were classified into multiple classifications.
 RESULTS
RESULTS
Based on the observations, process or process related comments and activities was a factor in 62% of the observations. The software solution was a factor in 54% of the observations and technology a factor in 39%. Remember, observations could be categorized into multiple categories.
The observations were further categorized by positive and negative sentiment, based on tone of voice, action or body language of the physician.Overall, there were 23% positive observations and 69% negative with 5% categorized as neutral. The positive results were highly skewed toward younger physicians or those who were computer savvy from any age group.
Some of the representative comments included:
 “I don’t have time for this; I will call from my phone to place orders.”
“I don’t have time for this; I will call from my phone to place orders.”- “I did not know I went to medical school to become a secretary.”
- “This is ridiculous!! All it does is take time away from my patients. I am with the patient now 5 minutes and with the computer 15 – 20 minutes.”
- “Something is going to get missed and someone is going to get hurt.”
- “I have not put orders in the computer for over 20 years and I am not starting now. I will retire before I start with this crap.”

Some of the representative behaviors included:
- Doctors would write orders on paper chart and leave for nurses to enter in system.
- Doctors were reluctant to ask for assistance (even though it was obvious they were having difficulties).
- A few doctors left the floor and then proceeded to call in the orders because they refused to place the orders themselves.
- A few doctors have slammed/pounded the keyboard in frustration.
- The nurses were getting very frustrated with doctors that didn’t enter their own orders (because they knew they would have to enter them for them).
An examination of the comments and behaviors, and many like them, reveals that the physicians’ comments and actions weren’t about the actual software solution, but about the process of actually entering in the orders. Getting physicians to overcome this hurdle will be critical in the success of any enterprise-wide transformation.
CONCLUSIONS
Based on these results, organizations might be overemphasizing technology to the detriment of good processes. This continuum misalignment can be illustrated by an inverted triangle as in the diagram below with the technology receiving the most emphasis and process receiving the least. A successful transformation involving technology must involve all three continuums equally. The choice and deployment of technology is just as important as training personnel which is just as important as the workflow design or redesign. Any attempt to do otherwise will result in failure. This failure could come in the form of poor physician acceptance, missed diagnosis information or unrecorded diagnosis information.

COMMENTARY
Healthcare is undergoing a period of tremendous change right now. The implementation of an EHR is only the first step in a long journey to becoming a data-enabled healthcare organization. Misalignment of any of the three continuums will minimize the chances for success. Neglecting the process continuum is especially risky.
Automating, or just adding technology, to bad process just results in a bad automated process. The same is true for not giving the process or workflow enough attention. This can be evident in challenges to personnel buy-in. A lot of times this occurs when the change is viewed as simply a software implementation as opposed to an organizational transformation. One rule to follow is the timing of initial training. If it is offered just before the software ‘goes live’ you have already failed. Organization transformation must start from the beginning with communication and personnel training throughout the process to increase acceptance and advocacy among the staff.
Physician engagement is an especially difficult challenge, but it can be overcome. Keeping physicians involved in the process and workflow design will improve buy-in and avoid rescinding a software workflow after it has been deployed because the process did not work or was inefficient for the physicians to utilize. It is critical to ‘get out in front’ of these issues because without all the clinical staff involvement the journey to become a data-enabled healthcare organization becomes more like the Tour de France, an endurance test through mountains, when it only needs to be the Chicago Marathon, an endurance test on city streets. There are obstacles and challenges, but there is no need to create mountains to climb.
OVERVIEW | METHODOLOGY | RESULTS | CONCLUSIONS | COMMENTARY